Type of Knee Ligament Injuries
Our knee is made up of many important structures, any of which can be injured. The most common knee injuries include fractures around the knee, dislocation, and sprains and tears of soft tissues, like ligaments. In many cases, injuries involve more than one structure in the knee.
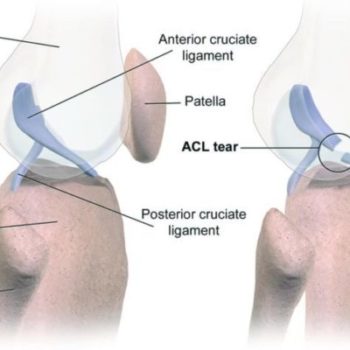
Anterior Cruciate Ligament (ACL) Injuries
The anterior cruciate ligament is often injured during sports activities. Athletes who participate in high demand sports like soccer, football, and basketball are more likely to injure their anterior cruciate ligaments. Changing direction rapidly or landing from a jump incorrectly can tear the ACL. About half of all injuries to the anterior cruciate ligament occur along with damage to other structures in the knee, such as articular cartilage, meniscus, or other ligaments.
Posterior Cruciate Ligament (PCL) Injuries
The posterior cruciate ligament is often injured from a blow to the front of the knee while the knee is bent. This often occurs in motor vehicle crashes and sports-related contact. Posterior cruciate ligament tears tend to be partial tears with the potential to heal on their own.