UPORTHOCON 2020
#UPORTHOCON_2020
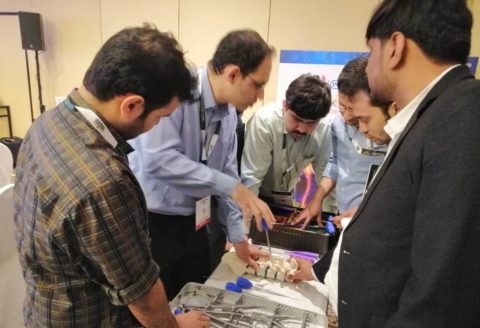
We participated in UPORTHOCON 2020 Event held in Golden Blossom Resort,Lucknow,UP on 14th to 16th February, 2020.
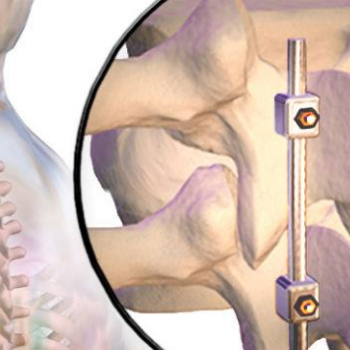
We exhibited our Orthopaedic Implants like Spinal Implants, Trauma Implants, Joints System and Surgical instruments.