What are the Most Common Types of Orthopedic Surgery?
An orthopedic surgery is any operation performed on the musculoskeletal system. This system is comprised of your bones, muscles, ligaments, joints and tendons. There are three different types of orthopedic surgery. Traditional procedures are now competing with minimally invasive arthroscopic surgeries that tout less pain and quicker recovery times.
Let’s take a look at the most commonly performed orthopedic procedures.
-
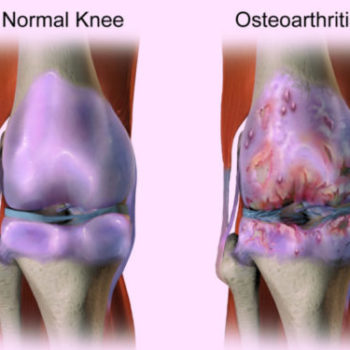
- Joint Replacement Procedures. These procedures replace an injured joint with a prosthetic and are among the most common orthopedic operations. Common joint replacement surgeries include hip and knee replacement surgeries. It is important that patients are monitored for signs of complications after these procedures because the procedures carry a considerable amount of risk. Among these risks are the chances that the implant will fail or that the materials making up the implant will make their way into the blood, causing a toxic condition known as metalosis.
-
- Revision Joint Surgery. If an existing implant has failed, it may be necessary to remove it and implant a new one. Revision surgeries are often required when the patient received a defective implant or an older implant has failed.
-
- Debridement. Whenever tissue death has occurred and the affected tissue needs to be removed before healing can occur, a debridement procedure is how doctors will remove it. There are some cases where bone is also removed when necessary.
-
- Spinal Fusion. Spinal fusions join the vertebrae together to provide more stability to the spine or to repair damage to the spine.
-
- Bone Fusion. Like spinal fusions, bone fusions use grafting to fuse fractured bones together so that they can heal.
-
- Soft tissue repair. These procedures focus on torn ligaments or tendons.
-
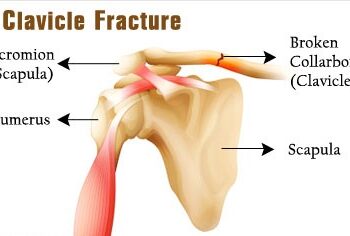
- Internal Fixation of Bones. This type of surgery places fragments of bones together and keeps them in place using pins, screws or plates so that they can heal. In some cases, the devices will remain inside of the body.
-
- Osteotomy. If a child has bone deformities, he or she will need this type of operation to help correct the deformity so that the bone grows properly.
From : www.rosenfeldinjurylawyers.com